The treatment of TGCT can be challenging and may include the use of medications. Sometimes TGCT cannot be entirely removed during surgery or the risk of complications from surgery outweighs the possible benefit. Other times TGCT recurs and patients are no longer amenable to surgery. A mix of anti-inflammatories, steroids, and pain medication can be given to manage the symptoms of TGCT; however, these do not treat the disease itself. In cases of either inoperable or recurrent TGCT, a medical oncologist can be a vital part of a healthcare team.
Surgery is often curative for localized TGCT due to the well-defined tumor boundary. This clear boundary allows the tumor to be completely removed during surgery (1). However, complete removal is not always possible. In diffuse TGCT, complete removal using surgery is more difficult due to the size of the tumor, the possibility of multiple loose bodies, and a lack of clear boundaries. In some cases of diffuse TGCT, following multiple surgeries, the tumors can recur again and again. Following the first recurrence, the risk of recurrence can increase. Repeated surgery can lead to secondary osteoarthritis and other health issues. Therefore, medications are available to treat patients with diffuse and/or recurrent TGCT.
***Note: Approved medications have two names, a brand name and a generic (or chemical) name. The generic or chemical name describes the drug itself while the brand name is intended to be catchy and make the drug more familiar. For example, Tylenol is the brand name for the drug acetaminophen. In TGCT, TURALIO is the brand name for Pexidartinib. These names are synonymous and refer to the same medication.
CSF-1 INHIBITORS
Genes dictate what proteins are made, like genetic blueprints. Every cell in our bodies have their own genetic blueprint. In TGCT, the TGCT cells produce excessive amounts of a protein called colony stimulating factor 1 (CSF1). The gene that is responsible for the production of CSF1 is located within a family, called the tyrosine kinase family. Like a family tree, other members of the tyrosine kinase family make proteins that look and act similar to each other. Proteins in this family function similarly and can be targeted in a similar way because they look similar. The medications that are intended to treat TGCT target the excessive production of CSF1, known as CSF1 inhibitors.
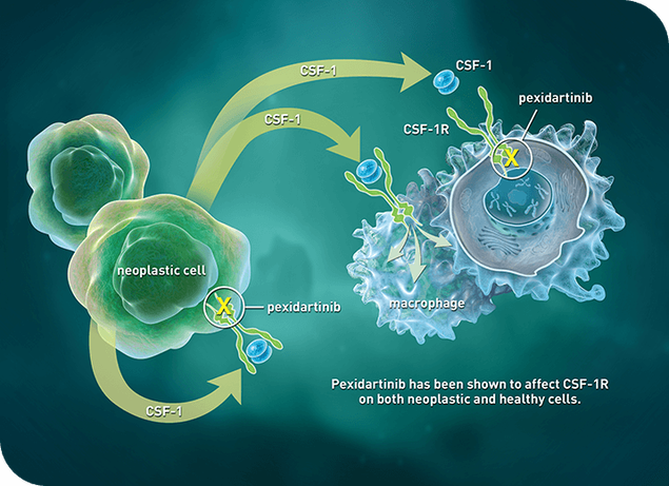
CSF1 inhibitors are a family of drugs that fall into a drug class called the tyrosine kinase inhibitors.Other tyrosine kinase inhibitors include nilotinib (Tasigna) and imatinib (Gleevec), which have been used off-label for the treatment of diffuse TGCT (2,3,4). Off-label means the medication was not originally made for this disease. TGCT uses the CSF1 protein to recruit other cells to become part of the tumor and grow. Since CSF1 is part of the same family as other tyrosine kinases, it can be targeted with medications already on market for other tyrosine kinase family members, like nilotinib and imatinib. These drugs act by disrupting the signaling between tumor cells and surrounding cells in the joint, halting tumor growth. Go to About TGCT to learn more about the biology of TGCT. Currently, there is a single drug approved in August 2019 for the treatment of recurrent and inoperable TGCT in the United States. This means that instead of targeting other members of the tyrosine kinase family to assert its anti-tumor activity, it directly targets CSF1 in TGCT and was made specifically for TGCT. TURALIO (Pexidartinib) is the first FDA-approved treatment for adults with symptomatic TGCT that is not amenable to improvement from surgery (5). Pexidartinib works by inhibiting CSF1 from signaling to TGCT and the surrounding cells. This disrupts the ability for the TGCT to recruit more cells, shrinking the tumor and halting the growth (6). Recently, it has been discovered that these treatments that blocks CSF1 at the cell source, such as Pexidartinib (Turalio) and Imatinib, target the surrounding immune cells being recruited and not the tumor cells themselves (7). This drug is only available in the United States under a risk mitigation program with the FDA. To learn more about TURALIO, go to Turalio.
It is recommended that if there is no approved treatment in your area, that clinical trials are considered for patients who may not benefit from surgery (8). A consensus document from experts exists that weighs the use of these medications, surgery, and active surveillance. To read this consensus document, go to Consensus Guideline.
For more information on on-going trials, go to Clinical Trials.
Ask your healthcare provider about CSF1 inhibitors available in your geographical location.
References
1. Nagase M, Araki A, Ishikawa N, et al. Tenosynovial Giant Cell Tumor, Localized Type With Extensive Chondroid Metaplasia: A Case Report With Immunohistochemical and Molecular Genetic Analysis. Int J Surg Pathol. 2020. doi:10.1177/1066896919889672 2. F.G.M. V, M.J.L. M, G. H, et al. Long-term efficacy of imatinib mesylate in patients with advanced Tenosynovial Giant Cell Tumor. Sci Rep. 2019. 3. Weaver C. Tenosynovial Giant Cell Tumor Treatment. Cancer Connect. https://news.cancerconnect.com/bone-cancer/tenosynovial-giant-cell-tumor-treatment-u1jsmV2RVUC1l6LHWX80Rg. Published 2019. 4. Gelderblom H, Pérol D, Chevreau C, et al. An open-label international multicentric phase II study of nilotinib in progressive pigmented villo-nodular synovitis (PVNS) not amenable to a conservative surgical treatment. J Clin Oncol. 2013. doi:10.1200/jco.2013.31.15_suppl.10516 5. FDA approves pexidartinib for tenosynovial giant cell tumor. Case Med Res. 2019. doi:10.31525/cmr-19c99e2 6. Pexidartinib for advanced tenosynovial giant cell tumor: results of the randomized phase 3 ENLIVEN study. The Lancet. 2020. DOI: 10.1016/S0140-6736(19)30764-0 7. David G.P.van IJzendoorn, MagdalenaMatusiak, et al. Interactions in CSF1-driven Tenosynovial Giant Cell Tumors. BioRxiv. 2022. DOI: 10.1101/2022.06.01.494428 8. Silvia Stacchotti et al. Best clinical management of tenosynovial giant cell tumour (TGCT): a consensus paper from the community of experts. Cancer treatment review. 2022. DOI: 10.1016/j.ctrv.2022.102491