TGCT can be diagnosed through MRI and/or biopsy. Often, TGCT presents with some unique imaging features that can distinguish it from other diseases. However, commonly, ruling out other more common diseases (differential diagnosis) is still required. Under a microscope, localized TGCT and diffuse TGCT look identical. However, these subtypes appear different on MRI images.
It is estimated that in 33% of diffuse TGCT patients, bone abnormality is observed(1). Additionally, cysts in non-weight bearing regions, such as Baker cysts, commonly accompany this disease.
Consult with your radiologist and multi-disciplinary healthcare team to interpret your results.
MRI features
Magnetic resonance imaging (MRI) allows for soft tissue to be visualized in the most clear and optimal way. A MRI is an imaging technique that utilizes a strong magnetic field and radio waves to generate an image that cannot be seen well on x-rays. MRI does not use radiation, instead, it relies on atoms in your body to align with the moving magnets in the scanner. MRI is an important tool to determine TGCT subtype, as described in Diagnosis. MRI images are broken down into components: T1, T2, and GRE. Each component tells the radiologist something about anatomical structures in that area.
Our body is made up of protons, neutrons, and electrons. The MRI creates an image by aligning protons with the magnetic field created by magnets moving in the scanner. T1 and T2 describe the relaxation time of the patients' protons under the MRI after different radiographic frequencies are pulsed. Different structures in our body create different relaxation times. For example, fat and bone have different relaxation times and show up differently on the MRI.
T2 is typically used to image chronic and progressive diseases compared to T1, which is the basic image produced by protons with a short relaxation time (2). Gradient recalled echo (GRE) is a type of spinning proton, leading to specific signals. For example, metal artifacts create low GREs. Because TGCT has hemosiderin, an iron-storing compound, radiologists can sometimes see a low GRE signal, low T1, and low T2 interval signal.
MRI results can be complex, consult with your radiologist and healthcare provider to go over MRI reports.
Localized
Localized TGCT often appears well-defined and discrete
Often stays within the joint space
Diffuse
Diffuse often appears wide spread with "homogenous", meaning of the same kind, soft tissue mass and an encompassing effusion (swelling)
Often extends outside the joint space
Hemosiderin deposits are seen as enhancements in the MRI, possibly giving a low GRE signal
"Blooming artifacts" are observed in 86% of diffuse patients and 27% of localized (3)
Intermediate to weak signal of T2 distinguishes TGCT from ganglion cysts, nerve-sheath tumors, and synovial sarcoma(4).
However, other diseases do cause weak to intermediate signal on MRI, making clinical correlation important
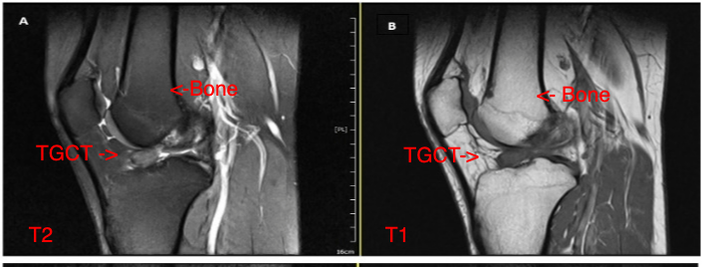
In A, T2 was used. The TGCT appears lighter than the knee bone. In B, T1 was used where the TGCT is darker than the neighboring bone.
Loiy Alkhatibm, Ralf Kraus, Scott, Sigman Ulrich Stahl, Loiy Alkhatibm. 2020. Tenosynovial Giant Cell Tumor in the Tibial Attachment of the Anterior Cruciate Ligament: A Case Report