For some patients, symptoms and clinical presentation may proceed diagnosis. Patients with TGCT often present with inflamed and thickened synovial tissue inside and/or outside the joint. Other symptoms include joint effusion (swelling), pain, stiffness, locking, tenderness, and limited range of motion. These symptoms are seen in other diseases, such as injury or synovial chondromatosis, and are significantly more common in other more prevalent diseases. This makes a differential diagnosis necessary for TGCT patients. A differential diagnosis means that the healthcare provider ruled out other possible diseases which led to the symptoms and pathology. Other diseases commonly misdiagnosed for TGCT can be found in Types of TGCT. Due to the many other more common diseases that have overlapping symptoms, the average time it takes a patient to be accurately diagnosed is around 3-4 years (1,2). However, symptoms can vary widely among patients, especially in localized TGCT versus diffuse TGCT. Patients with diffuse TGCT are more likely to exhibit severe symptoms, while localized TGCT patients may have more mild symptoms. This may not always be the case. In some cases, diffuse TGCT patients may present with mild symptoms while localized TGCT patients may have severe symptoms. The “typical” presentation of this disease is often hard to predict. Therefore, patients medical history and physical examination are crucial for the right diagnosis.
Imaging Modalities
The preferred imaging used in the diagnosis of TGCT and monitoring post operatively are magnetic resonance imaging (MRI) with or without contrast dye. However, patients also often have other forms of radiography to support their diagnosis or treatment. Each imaging technique provides strengths and weaknesses depending on the intent.
X-Ray
In daily life, the most common radiology technique is radiography. Radiography uses x-rays to view internal structures of the body, mostly skeletal. X-rays use a type of radiation known as electromagnetic waves which will produce an image on metal film. Soft tissue, such as skin and organs, cannot absorb the electromagnetic waves and allow the high energy to pass through them. Once the high energy waves reach bone and other solid structures, the radiation will be absorbed allowing an image of those regions. X-rays are the least expensive of the imaging techniques and generally the quickest. Degeneration, effusion, bone erosion, and the amount of joint space can be identified on x-ray, giving a quick snapshot of what may be going on internally. However, x-rays do not show soft tissue, therefore, tumors cannot be visualized using x-rays. In order to understand what is leading to the potential effusion, bone erosion, and damage to the joint space, an MRI must be used.
Magnetic resonance imaging
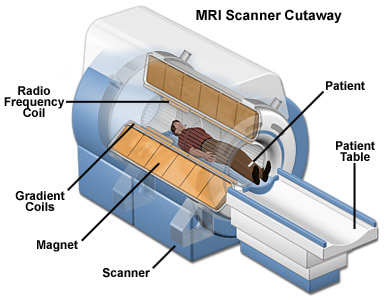
Magnetic resonance imaging (MRI) are the preferred and recommended diagnostic and monitoring imaging for patients with TGCT. MRI allows for soft tissue to be visualized in the most clear and optimal way. MRI utilizes a strong magnetic field and radio waves to generate an image that cannot be seen well on x-rays. MRI does not use radiation, instead, it relies on atoms in your body to align with the moving magnets in the scanner. During a MRI scan, radiofrequencies are pulsed through a patient allowing their atoms to move according to the magnets. This alignment with the magnets leads to an image shown in T1 and T2 intervals. The joint can be easily depicted during an MRI. T2 intervals refer to the appearance of fluid, often in this case, synovial fluid and effusions. TGCT patients often have swelling leading to excess T2 intervals present. TGCT tumors are soft tissue tumors that require a blood supply to receive nutrients and grow. Because of this blood supply to the tumor, they also show up on T1 intervals. This allows easy determination of the tumors if the radiologist has experience in this diagnosis. Often times the MRI is coupled with contrasting dye. The contrasting dye injected, either locally into the joint via arthrogram or through an intravenous injection. Most commonly, contrast dye is a gadolinium-based dye. This dye enhances the quality of the imaging and enables radiologists to more confidently identify soft tissue tumors. The contrasting dye temporarily enhances the T1 intervals, leading to more accurate diagnostics. Specifically, contrast agent is added to scans to visualize tumors, inflammation, certain organ's blood supply, and blood vessels. Not every MRI will require contrasting dye. Your healthcare provider will determine whether to add contrast or not based on your present condition and your health history.
To learn more about MRI features of this disease, go to Imaging Features
Computed tomography (CT scan)
Computed Tomography, commonly referred to as a CT scan, is an imaging technique that utilizes a combination of x-rays and a computer to create a picture of organs, bone, and other tissues. A series of images are taken using x-rays at different angles around the body, giving more 3 dimensional information. This technique allows for more accuracy than a x-ray, however, the image is less clear than a MRI. Therefore, a MRI is most often used.
References
1. Bhimani MA, Wenz JF, Frassica FJ. Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop Relat Res. 2001. doi:10.1097/00003086-200105000-00025 2. Stephan SR, Shallop B, Lackman R, Kim TWB, Mulcahey MK. Pigmented villonodular synovitis: A comprehensive review and proposed treatment algorithm. JBJS Rev. 2016. doi:10.2106/JBJS.RVW.15.00086