Localized/nodular |
|
|
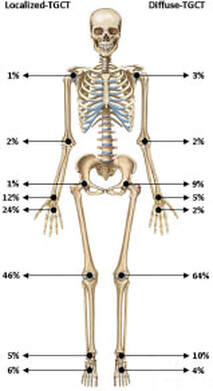
The localized form of TGCT is the most prevalent, with 85-90% of the TGCT diagnoses (6)
|
Mastboom MJL, Verspoor FGM, Verschoor AJ, et al. Higher incidence rates than previously known in tenosynovial giant cell tumors. Acta Orthop. 2017.
|
The diffuse form of TGCT is less common, and 2.6 times more likely to recur (7)
|
Localized/nodular |
|
Localized/Nodular |
|
|
|