Also known as pigmented villonodular synovitis (PVNS) and giant cell tumor of the tendon sheath (GCT-TS)
TGCT is a type of rare, locally aggressive, non-life threatening, tumor of the joint, tendon sheath, or bursae. TGCT leads to stiffness, pain, swelling, and limited range of motion in the affected joint (1). In 2013, The World Health Organization reclassified giant cell tumor of the tendon sheath (GCT-TS), nodular tenosynovitis, pigmented villonodular synovitis (PVNS), and diffuse-type giant cell tumor as a single disease entity known as Tenosynovial Giant Cell Tumor (TGCT) with two subtypes. There are two subtypes of TGCT, localized and diffuse (2). Localized/Nodular TGCTencompasses previously named nodular tenosynovitis and GCT-TS, while Diffuse TGCT includes diffuse-type giant cell tumor and PVNS. The type of TGCT often influences recurrence risk and treatment options. Learn more about the subtypes at Types of TGCT.
TGCT varies in clinical presentation and can occur at all ages (3). According to NORD, the disease commonly presents in people 25-50 years of age, while diffuse TGCT tends to occur in those < 40 years old (4). TGCTs are rare and researchers don’t know exactly how many people are diagnosed with TGCT each year. However, a study done in the Netherlands was used to calculate the worldwide incidence. Globally, it is estimated that 43 people out of every million are newly diagnosed with TGCT, localized and diffuse forms, each year (5). However, a Danish study found that 44 per 100,000 people are currently living with localized TGCT and 12 per 100,000 people are living with diffuse TGCT (6). More people are living with the disease than newly diagnosed because this number includes those newly diagnosed and those who have had it long-term.
Surgery may be curative for many people with TGCT, but for others, TGCT may recur after surgery. Recurrence rates depend on the subtype of TGCT (6). Different types of doctors are likely to be involved in the care of patients with TGCT. For hard-to-treat cases, care teams should include sarcoma specialists. These doctors have experience treating difficult tumors similar to TGCT.
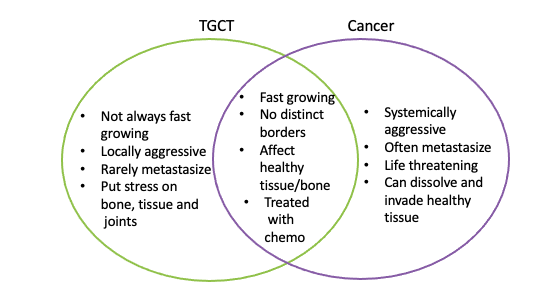
The World Health Organization classifies these tumors as "intermediate tumors". This means that these tumors rarely spread and are locally aggressive (7). These tumors are benign but may share similar features to soft tissue cancers, also referred to as sarcoma. It is important to note that these tumors are not cancerous. For example, TGCT puts stress on local bones, tissue, and joints but does not spread; whereas, sarcomas can spread to healthy tissue in distant locations. There is no such thing as a good tumor; however, TGCT is rarely life threatening, unlike cancer. TGCT and sarcoma share some characteristics, such as, both can lead to severe functional impairment when left untreated. Joint deterioration can drastically impact quality of life in patients with TGCT. TGCT, especially the diffuse type, can lack a distinct boundary making complete surgical resection difficult. Additionally, these tumors may be treated with drugs that are targeted to the tumor, such as Pexidartinib (Turalio). The best treatment modality is highly debated and should be based on an individualized approach that fits the needs of the patient. Additional treatments are being investigated and research is bridging the knowledge gaps to improve the understanding of which patients would benefit from which specific treatments. To learn more about treatments, go to Treatment.
What makes up tGCT tumors?
There are hundreds of different types of cells in the body. All of these different cells serve a specific and diverse function. The cells within a TGCT are just as diverse. Tumors can begin in almost any type of cells in the body.
The type of cell defines the biology of the tumor and the location can influences the treatment plan. The types of cells in these tumors include fibroblasts, monocytes, macrophages, and giant cells. Fibroblasts: Fibroblasts are a type of cell that make up connective tissue, often in ligaments and tendons (8). They are found throughout the body as structural support for our organs. Monocytes & Macrophages: Monocyte are a type of white blood cell that can function as a macrophage. A macrophage is a specialized white blood cell involved in the inflammatory response. These white blood cells remove dead cells, kill microorganisms (eg. like infections), and recruit other cells. A portion of the TGCT is made up of tumor cells while the rest of the tumor is made up of monocytes and macrophages that become part of the tumor.
The TGCT promotes the growth and recruitment of these cells to become part of the tumor.
Multi-nucleated Giant Cells: These cells formed by the joining of monocytes and macrophages to become a single cell. These cells are often associated with the soft tissue and bone damage. These cells are large and mediate tissue repair and remodeling. However in TGCT patients, only 2-16% of the tenosynovial giant cells have a genetic abnormality that provokes tumor growth (9).
1. Gelhorn HL, Tong S, McQuarrie K, et al. Patient-reported Symptoms of Tenosynovial Giant Cell Tumors. Clin Ther. 2016. doi:10.1016/j.clinthera.2016.03.008 2. Righi A, Gambarotti M, Sbaraglia M, et al. Metastasizing tenosynovial giant cell tumour, diffuse type/pigmented villonodular synovitis. Clin Sarcoma Res. 2015. doi:10.1186/s13569-015-0030-2 3. Healey JH, Bernthal NM, van de Sande M. Management of Tenosynovial Giant Cell Tumor: A Neoplastic and Inflammatory Disease. J Am Acad Orthop Surg Glob Res Rev. 2020. doi:10.5435/JAAOSGlobal-D-20-00028 4. National Organization for Rare Disorders. Tenosynovial Giant Cell Tumor. NORD. 2017. https://rarediseases.org/rare-diseases/tenosynovial-giant-cell-tumor/. 5. Mastboom MJL, Verspoor FGM, Verschoor AJ, et al. Higher incidence rates than previously known in tenosynovial giant cell tumors. Acta Orthop. 2017. 6. Ehrenstein V, Andersen SL, Qazi I, et al. Tenosynovial Giant Cell Tumor: Incidence, Prevalence, Patient Characteristics, and Recurrence. A Registry-based Cohort Study in Denmark. J Rheum. 2017. https://www.jrheum.org/content/44/10/1476.long 7. Levin A. Tenosynovial Giant Cell Tumor: A New Name and a New Treatment Option for PVNS and GCTTS. Am Acad Orthop Surg. 2021. https://www.aaos.org/aaosnow/2021/jan/research/research01/. 8. Al Saanna G, Bovée J, Hornick J, Alexander Lazar A. A Review of the WHO Classification of Tumours of Soft Tissue and Bone. ESUN B Rev. 2013. http://sarcomahelp.org/reviews/who-classification-sarcomas.html. 9. Hügel H. Fibrohistiocytic skin tumors. JDDG - J Ger Soc Dermatology. 2006. doi:10.1111/j.1610-0387.2006.06021.x 10. Gouin F, Noailles T. Localized and diffuse forms of tenosynovial giant cell tumor (formerly giant cell tumor of the tendon sheath and pigmented villonodular synovitis). Orthopaedic and Traumatology: Surgery & Research. 2017. doi: 10.1016/j.otsr.2016.11.002