Arthroscopy |
|
|
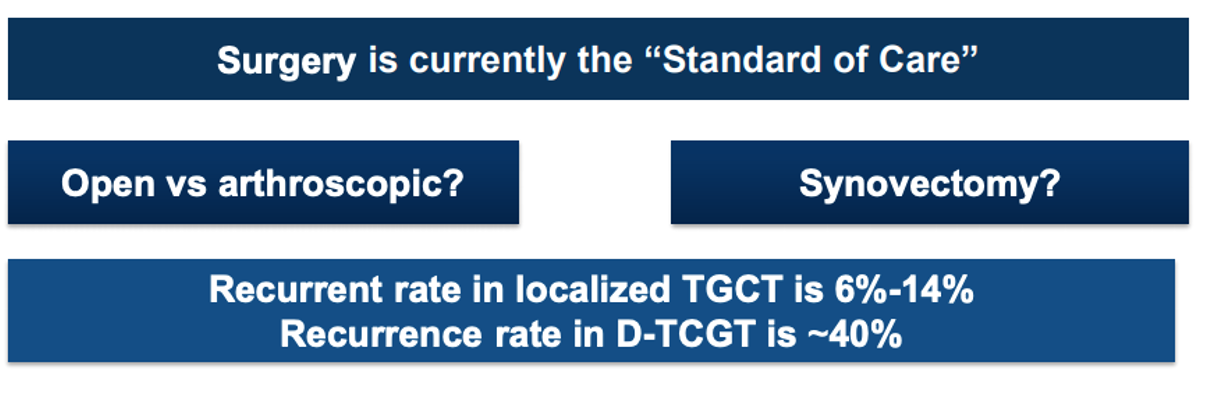
In both diffuse and localized/nodular TGCT, arthroscopic surgery can be used to remove the damaged joint lining. This approach uses a few small incisions around the joint with one incision used to insert a camera, known as the the arthroscope. The arthroscope allows the surgeon to see the joint lining projected on a larger screen to guide the other surgical instruments (1). In many localized/nodular TGCT cases, this surgery is curative. Arthroscopic surgeries may involve shorter recovery time and hospital stays.
|
In diffuse TGCT, open surgery can be used based on the accessibility of the tumor location, size of tumor, and extent of the damage in the joint. The open surgery uses a single large incision to gain full access to the joint to remove the tumor and synovial tissue. Depending on the tumor location, joint dislocation may be required to gain access (like in the case of the hip) (2). Open surgeries may require longer hospital stays and longer recovery time.
|
|

|